
Topics
10/14/2024
The Growing Importance of Body-Weight Set Point Theory: How Can the Recent Rise in Obesity Be Explained?
Summary
(1)The body weight set point model
In 1953, Gordon C. Kennedy proposed that the accumulation of body fat may be physiologically regulated. Later, in 1982, nutritionists William Bennett and Joel Gurin expanded on this concept and developed the “set-point theory.”
(2)Body-weight homeostasis
When an individual loses weight, the body not only reduces energy expenditure beyond what would be predicted from changes in body composition and the thermic effect of food, but also increases appetite through hormonal regulation and alters food preferences. As a result, conditions are created that make weight rebound more likely.
In contrast, temporary weight gain caused by overeating is also thought to trigger compensatory mechanisms that act to return body weight toward its set-point range. However, these mechanisms may be weaker than those that resist weight loss.
A person’s body-weight set point is thought to be established from childhood through adolescence and to remain relatively stable thereafter. However, it has also been suggested that it may shift in response to major environmental changes such as marriage, childbirth, or migration.
Currently, set-point theory has become an important framework for explaining why body weight is not regulated solely by willpower or simple calorie calculations.
(3)Limitations of the set-point model
The set-point model, which proposes that body weight is regulated within a certain range, does not fully explain the sharp rise in obesity observed primarily in Western countries since the 1970s. In response to this limitation, some researchers have suggested that while metabolic resistance to maintaining weight loss is strong, physiological resistance to sustained fat gain may not persist over the long term.
(4)Questions regarding the high-energy diet hypothesis
Animal studies have reported irreversible weight gain following the long-term consumption of high-energy diets. In humans, however, some individuals remain lean despite consuming similarly high-calorie diets, and the hypothesis does not readily account for phenomena such as weight gain associated with social class or major environmental changes.
(5)Intestinal starvation as an alternative perspective
The recent rise in obesity cannot be fully explained by excess energy intake alone. Irreversible weight gain reflecting an upward shift in the body-weight set point may instead be triggered when the body perceives that “food is scarce.”
Since the 1970s, advances in food processing and the resulting changes in the food environment may have increased the likelihood of a physiological state in which the body perceives that ingested food has been completely digested within the intestinal tract—what I refer to as “intestinal starvation.”
【 Full text 】
-
Contents
-
- Advances in understanding set-point theory
- Limitations of the set-point model
- Environmental and behavioral factors influencing the body-weight set point
I view the human body as possessing a homeostatic system that attempts to maintain body weight within a certain range, and from this perspective, I believe that the concept of a body-weight set point carries important implications.
In this article, I will discuss the background and challenges of set-point theory, which has received renewed attention in recent years. I believe that understanding the environmental and behavioral factors that may contribute to upward shifts in the body-weight set point is important for addressing the growing problem of obesity.
1. Advances in understanding set-point theory
Obesity and weight loss attempts
♦An obese individual who insists that a lean friend has consistently eaten more than the fat person does, may well be telling the truth.(*snip*)
The group of obese patients who are greatly in need of our understanding are those who keep to a calorie intake of perhaps 1,000 kcal per day, yet lose less than one kg per week. There is no doubt whatsoever that such people exist, and can be studied in a metabolic ward under conditions where 'cheating' is virtually impossible without being detected.
Usually these are middle-aged women who have been perhaps 40 kg overweight, and who have already lost about 20 kg. They are often depressed, hypothermic, and have a low metabolic rate. The nature of this metabolic adaptation to a low-calorie diet is not known (as of 1973), but it is a phenomenon that has been recognized since before the 1920s (J S Garrow, 1973)[1].
♦For obese individuals, a certain amount of weight loss is possible through a range of treatments, but long-term maintenance of weight loss is much more challenging, and in most cases, the weight is regained [2]. In a meta-analysis of 29 long-term weight loss studies, more than half of the lost weight was regained within two years, and by five years, more than 80% of lost weight was regained [3,4].
In addition, studies of those who are successful at sustained weight loss indicate that the maintenance of reduced body fat will probably require close attention to energy intake and expenditure, perhaps for life [5].
Energy expenditure in obesity
♦The hypometabolic thesis had fallen out of favor by 1930, when more accurate calculations of body-surface area indicated that the metabolic rates of obese individuals were normal [6].
♦Total energy expenditure (TEE) in a day consists of three components: diet-induced thermogenesis (DIT), physical activity energy expenditure (PAEE), and resting energy expenditure (REE).
When comparing hypothetical men weighing 100 kg and 70 kg, the man weighing 100 kg has a higher TEE [7].
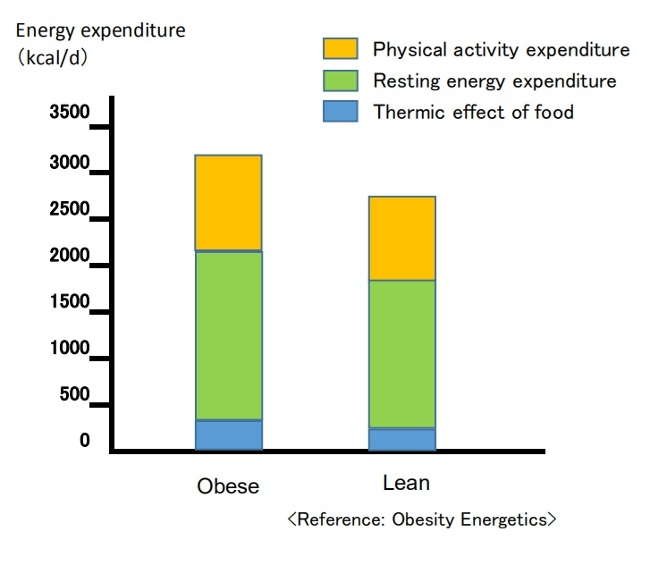
Breakdown of energy expenditure in average 100-kg and 70-kg men
Contrary to popular belief, people with obesity generally have a higher absolute REE compared to leaner subjects. This is because obesity increases both body fat and metabolically active fat-free mass [7,8].
PAEE can be subdivided into "voluntary exercise" and “activities of daily living.” Despite typically engaging in less physical activity, obese individuals often have a daily energy cost for physical activity similar to that of non-obese individuals since PAEE is proportional to body weight [7,9]. Additionally, due to greater food intake, their DIT also tends to be higher [7].
Dynamic changes in energy expenditure
♦Obesity prevention is often erroneously described as a simple bookkeeping matter of balancing caloric intake and expenditure [10].
In this model, energy intake and expenditure are considered independent parameters determined solely by behavior. It is assumed that an obese person can steadily lose weight by eating less and/or moving more at a rate of one pound for every 3,500 kcal (or one kg for every 7,200 kcal) of accumulated dietary caloric deficit [7,11]. This view has been referred to as a “static model” of weight loss, but it has been shown to be physiologically impossible [7,12].
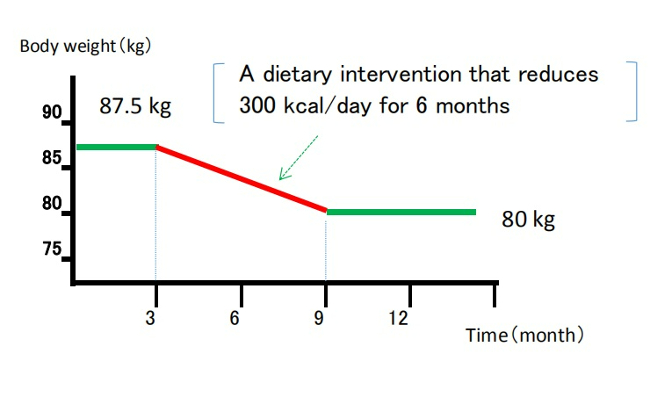
Static model of weight loss
(Despite being recognized as overly simplistic, the 3,500 kcal rule continues to appear in scientific literature and has been cited in over 35,000 educational weight-loss websites as of 2013.) [12,13]
♦It is now understood that energy intake and expenditure are interdependent variables, influenced by each other and by homeostatic signals triggered by changes in body weight [7,14].
Attempts to alter energy balance through diet or exercise are countered by physiological adaptations that resist weight loss [7].
Body weight set point theory
♦In recent years, the influence of homeostatic control has become increasingly recognized, and growing evidence suggests that the body employs physiological mechanisms to regulate energy balance and maintain body weight around a genetically and environmentally determined set point [12].
In 1953, Kennedy proposed that body fat storage is regulated [15]. In 1982, nutritional researchers William Bennett and Joel Gurin expanded on Kennedy's concept when they developed the set-point theory [16]. The model has been widely adopted, and strengthened particularly after the discovery of leptin in the 1990s [7,12].
When an individual loses weight, the body significantly reduces energy expenditure to a degree that is often greater than predicted based on changes in body composition or the thermic effect of food. This process also causes an increase in appetite through hormonal regulation and alters food preferences through behavioral changes, to drive body weight back toward its set-point range[7,16].
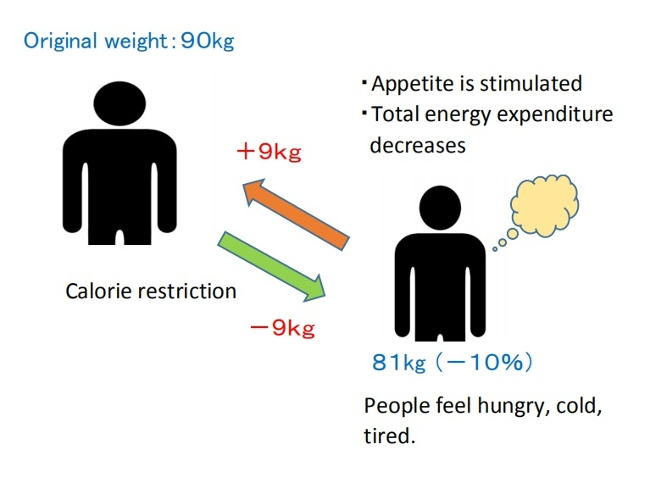
Set-point model of weight loss
♦Weight-loss studies have shown that the magnitude of fat stores in the body is protected by mechanisms mediated by the central nervous system, which adjust energy intake (EI) and expenditure (EE) via signals from adipose tissue, the gastrointestinal tract, and endocrine organs to maintain homeostasis and resist weight change as proposed by the set-point model [12,17].
♦The body's protective metabolic mechanism that attempts to preserve energy stores during an energy crisis is known as adaptive thermogenesis (AT) or metabolic adaptation [7,12].
AT is defined as the underfeeding-associated fall in resting energy expenditure (REE), independent of changes in body composition [12].
♦Maintenance of a 10% or greater reduction in body weight in lean or obese individuals is accompanied by about 20 to 25% decline in 24-hour energy expenditure. This decrease in weight maintenance calories is 10–15% greater than predicted based solely on changes in fat and lean mass [17,18].
Since obese individuals also display these compensatory metabolic adjustments in response to dietary restriction, obesity may be considered a natural physiological state for some people. Experimental studies on obesity in animals similarly suggest a view of obesity as a condition of body energy regulation at an elevated set point [19].
♦A meta-analysis of cross-sectional studies investigating adaptive thermogenesis (AT) by comparing formerly obese subjects who had lost weight with BMI-matched subjects who were never obese, found a 3–5% lower resting energy expenditure (REE) in formerly obese subjects compared to never obese controls [20].
This effect means, for example, that if an obese woman reduced her weight from 100 kg to 70 kg, she would have to consume fewer calories to remain at 70 kg than a woman who had consistently weighed 70 kg [6]. Similar results have been confirmed in animal experiments involving obese and normal-weight rats.
This suggests that the frequent claim made by obese people that they eat the same or less than their lean friends but lose no weight, must be given more credence than it is ordinarily accorded [19].
♦On the other hand, as shown in overfeeding experiments on prisoners in Vermont in the 1960s (Doctor Ethan Sims), weight gain due to temporary overeating also triggers compensatory mechanisms that bring body weight back toward its set-point range.
However, some researchers point out that these may be weaker than the mechanisms that resist weight loss.
This asymmetry could be due to the evolutionary advantage of storing fat to survive during periods of food scarcity or starvation [16,17].

♦In addition, hyperphagia (overeating) has been demonstrated following experimental semi-starvation and short-term underfeeding, which is probably the result of homeostatic signals resulting from the loss of both body fat and lean tissue [7,21].
♦This theory also suggests that a person's body-weight set point is established early in life and remains relatively stable unless altered by specific conditions. However, the set point may change throughout one’s life due to factors such as marriage, childbirth, menopause, aging, and disease [16].
On the other hand, the set-point theory remains hypothetical because the molecular mechanisms involved in set-point regulation have not yet been fully elucidated, and some researchers may consider the theory overly simplistic [16].
2. Limitations of the set-point model
On the other hand, some researchers have pointed out important limitations of the body-weight set-point model.
If a homeostatic system truly exists to maintain body weight within a certain range, a fundamental question arises: why do so many individuals in Western countries continue to gain weight gradually throughout majority of their adult lives? In particular, this model does not adequately explain the increasing prevalence of obesity observed in many societies worldwide since around the 1970s [22].
In response, some researchers have suggested that while metabolic resistance to sustaining a reduced body weight is strong, metabolic resistance to sustained increased adiposity may not be physiologically long-lasting. Indeed, the steady increase in obesity prevalence supports the idea that the human body may be physiologically more permissive of weight gain than of weight loss [17,23].
■Animal studies using rats have shown that during the first 3–4 weeks of exposure to a high-fat diet, increases in energy expenditure and activation of the sympathetic nervous system (SNS) can be observed.
However, these compensatory responses were no longer evident after a few months of high-fat diet consumption [17,24].
Furthermore, another rat study has reported that long-term consumption of highly palatable, high-energy diet—such as potato chips and cheese crackers—led to irreversible weight gain, suggesting an upward shift in the body-weight set point [19,25].

These explanations that continuous consumption of high-calorie diet leads to an increase in the body-weight set point may sound plausible at first. However, in my opinion, if body weight changes in only one direction in response to a single external factor, it can no longer be considered a true “set point.”
Moreover, when this hypothesis is applied to humans, it fails to account for the fact that some individuals remain lean despite frequently consuming similarly high-calorie foods. In practice, several contradictions can be identified, including the following:
(1) Obesity is frequently observed among low-income populations in Western countries, as well as among relatively affluent groups in developing countries [22, 27, 28].
(2) Since the 1950s, the coexistence of undernutrition and obesity within poor populations has been documented worldwide [29].
(3) A substantial number of individuals gain weight following major life or environmental changes—such as entering university, marriage, childbirth, or migration from Asia to Western countries [22].
I propose that upward shifts in the body-weight set point are associated with adaptive responses to intestinal starvation.
The next section provides a more detailed explanation of this mechanism.
3. Environmental and behavioral factors influencing the body-weight set point
At present, many international organizations classify obesity as a chronic disease.
Some researchers interested in the body-weight set-point theory have argued that determining whether obesity, as a chronic condition, is treatable requires a clear understanding of how genetic and environmental factors interact to regulate the set point. At the same time, it is also true that many important environmental and social influences remain insufficiently explained [22].
In this article, I will introduce the concept of “intestinal starvation” as a complementary perspective to address these challenges. The key points are outlined below in four parts.
(1) Limitations of the positive energy balance hypothesis
It is generally assumed that weight gain requires a positive energy balance, and the recent rise in obesity is often explained by increased consumption of high-calorie foods and reduced levels of physical activity. Paradoxically, however, the fact that obesity rates have increased in parallel with the growing prevalence of dieting aimed at weight loss [30] suggests that our current understanding of energy balance may warrant reconsideration [12].
What I want to emphasize is that while short-term weight gain due to overeating can be explained by excess energy intake, long-term and potentially irreversible weight gain may instead be triggered by energy deprivation or by the body’s perception that food is scarce. This pattern is also consistent with the phenomenon in which body weight increases beyond its previous level following experimental starvation or weight-loss dieting.
【Related Articles】The Spread of Dieting May Be Fueling the Rise in Obesity
(2) Changes in digestion and absorption brought about by food processing
It is certainly true that high-calorie foods have become increasingly common since the 1970s. However, an even more important factor affecting the human body may be the rise of food processing—particularly ultra-processing. As food processing advanced, hard-to-digest components were gradually removed, while softer and more easily digestible components became increasingly dominant.

As a result, substantial changes may have occurred in the rate of digestion and absorption, as well as in the gut environment.
Intestinal starvation appears to be associated with the frequent consumption of refined carbohydrates and (ultra-)processed foods, and may help explain both the rise in obesity since the 1970s and why obesity can occur frequently not only in developed countries, but also in certain regions of the developing world.
【Related Article】
The Rise in Obesity is Closely Linked to the Consumption of Ultra-Processed Foods
(3) Intestinal starvation as a multifactorial model
Intestinal starvation is a physiological state that is more likely to occur when four factors overlap simultaneously. This concept provides a framework for understanding obesity as a chronic condition arising from interactions between genetic and environmental factors.
【Related Article】Three (+1) Factors That Accelerate “Intestinal Starvation”
(4) Why does the body resist weight loss in obese individuals?
In cases of weight gain that may reflect an upward shift in the body-weight set point through intestinal starvation, the overall efficiency of nutrient absorption may increase. In other words, from the perspective of energy homeostasis, the balance point at which energy intake and expenditure are matched may itself shift to a higher level. This perspective may help explain why even obese individuals with substantial body fat often exhibit compensatory metabolic responses to caloric restriction.
【Related Article】How Intestinal Starvation Can Lead to Weight Gain
As mentioned in the section 2, an animal study in rats reported that 90 days of exposure to a “high-energy diet” resulted in irreversible weight gain suggestive of an upward shift in the body-weight set point (Rolls et al., 1980). However, the “fattening diet” used in this experiment consisted mainly of commercially available, highly palatable foods such as potato chips, cheese crackers, and cookies [25]. At the same time, these foods were also highly refined carbohydrates and (ultra-)processed foods.
In contrast, the solid chow provided to the control group consisted of cracked grains, soybean meal, fish meal, and similar ingredients, and may have contained larger amounts of less digestible matter, such as dietary fiber and the tough cell walls of plants. In this respect, the composition of the control diet may have resembled that of human diets commonly seen more than 50 years ago.
Therefore, I believe that caution is needed before concluding that the long-term consumption of a high-energy diet directly caused weight gain suggestive of an upward shift in the body-weight set point.
<References>
[1]Garrow JS. Diet and obesity. Proc R Soc Med. 1973 Jul;66(7):642-4. PMID: 4741395; PMCID: PMC1645095.
[2]Wu T, Gao X, Chen M, van Dam RM. Long-term effectiveness of diet-plus-exercise interventions vs. diet-only interventions for weight loss: a meta-analysis. Obes Rev. 2009;10(3):313–323.
[3] Hall KD, Kahan S. Maintenance of Lost Weight and Long-Term Management of Obesity. Med Clin North Am. 2018 Jan;102(1):183-197.
[4]Anderson JW, Konz EC, Frederich RC, Wood CL. Long-term weight-loss maintenance: a meta-analysis of US studies. Am J Clin Nutr. 2001 Nov;74(5):579-84.
[5]Wing RR, Hill JO. Successful weight loss maintenance. Annu Rev Nutr. 2001;21:323-41.
[6]Jou C. The biology and genetics of obesity--a century of inquiries. N Engl J Med. 2014 May 15;370(20):1874-7.
[7]Hall KD, Guo J. Obesity Energetics: Body Weight Regulation and the Effects of Diet Composition. Gastroenterology. 2017 May;152(7):1718-1727.e3.
[8]Nelson KM, Weinsier RL, Long CL, et al. Prediction of resting energy expenditure from fat-free mass and fat mass. Am J Clin Nutr. 1992;56:848–856.
[9]Westerterp KR. Physical activity, food intake, and body weight regulation: insights from doubly labeled water studies. Nutr Rev. 2010;68:148–154.
[10] Levine DI. The curious history of the calorie in U.S. policy: a tradition of unfulfilled promises. Am J Prev Med. 2017;52:125–129.
[11] Hall KD, Chow CC. Why is the 3500 kcal per pound weight loss rule wrong? Int J Obes (Lond). 2013 Dec;37(12):1614.
[12] Egan AM, Collins AL. Dynamic changes in energy expenditure in response to underfeeding: a review. Proc Nutr Soc. 2022 May;81(2):199-212. doi: 10.1017/S0029665121003669. Epub 2021 Oct 4. PMID: 35103583.
[13]Thomas DM, Martin CK, Lettieri S et al. (2013) Can a weight loss of one pound a week be achieved with a 3500-kcal deficit? Commentary on a commonly accepted rule. In Int J Obes 37, 1611–1613.)
[14]Hall KD, Heymsfield SB, Kemnitz JW et al. Energy balance and its components: implications for body weight regulation. Am J Clin Nutr. 2012 Apr;95(4):989-94.
[15]KENNEDY GC. The role of depot fat in the hypothalamic control of food intake in the rat. Proc R Soc Lond B Biol Sci. 1953 Jan 15;140(901):578-96.
[16] Ganipisetti VM, Bollimunta P. Obesity and Set-Point Theory. 2023 Apr 25. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan–. PMID: 37276312.
[17] Rosenbaum M, Leibel RL. Adaptive thermogenesis in humans. Int J Obes (Lond). 2010 Oct;34 Suppl 1(0 1):S47-55.
[18] Leibel R, Rosenbaum M, Hirsch J. Changes in energy expenditure resulting from altered body weight. N Eng J Med. 1995;332:621–28.
[19] Richard E. Keesey, Matt D. Hirvonen, Body Weight Set-Points: Determination and Adjustment, The Journal of Nutrition, Volume 127, Issue 9, 1997, Pages 1875S-1883S, ISSN 0022-3166.
[20]Astrup A, Gøtzsche PC, van de Werken K, et al. Meta-analysis of resting metabolic rate in formerly obese subjects. Am J Clin Nutr. 1999 Jun;69(6):1117-22.
[21] Dulloo AG, Jacquet J, Girardier L. Poststarvation hyperphagia and body fat overshooting in humans: a role for feedback signals from lean and fat tissues. Am J Clin Nutr. 1997;65:717–723.
[22]Speakman JR, Levitsky DA, Allison DB, et al. Set points, settling points and some alternative models: theoretical options to understand how genes and environments combine to regulate body adiposity. Dis Model Mech. 2011 Nov;4(6):733-45.
[23] Schwartz MW, Woods SC, Seeley RJ, et al. Is the energy homeostasis system inherently biased toward weight gain? Diabetes. 2003 Feb;52(2):232-8.
[24] Corbett SW, Stern JS, Keesey RE. Energy expenditure in rats with diet-induced obesity. Am J Clin Nutr. 1986 Aug;44(2):173-80.
[25] Rolls B.J., Rowe E.A., Turner R.C. Persistent obesity in rats following a period of consumption of a mixed high energy diet. J Physiol. 1980 Jan;298:415-27.
[26](Deleted)
[27] Dykes J et al. Socioeconomic gradient in body size and obesity among women: the role of dietary restraint, disinhibition and hunger in the Whitehall II study. International Journal of Obesity 2004 Feb,:262-68.
[28] Poskitt EM. Countries in transition: underweight to obesity non-stop? Ann Trop Paediatr. 2009 Mar;29(1):1-11.
[29] Gary Taubes. 2011. Why we get fat. New York: Anchor Books. Pages 15-32.
[30] Montani JP, Schutz Y, Dulloo AG. Dieting and weight cycling as risk factors for cardiometabolic diseases: who is really at risk? Obes Rev. 2015 Feb;16 Suppl 1:7-18.