
— Topics —
How you eat (Way of intake)
2025.08.15
The Spread of Dieting May Be Fueling the Rise in Obesity
Summary
(1) The prevalence of dieting has increased over the past several decades, paralleling the rising prevalence of overweight and obesity. This has raised concerns that dieting may, paradoxically, be contributing to obesity.
(2) Some observational studies suggest that the association between dieting and weight gain may be at least partly causal. However, some researchers argue that dieting is merely a proxy marker for a tendency to overeat.
(3) Several prospective studies have suggested that dieting for weight loss among adolescents, middle-aged women, and even individuals of normal weight is a strong predictor of future weight gain.
(4) In studies of adolescents, boys and girls who continued unhealthy weight-control behaviors—such as fasting, skipping meals, eating very little, or using food substitutes—showed the greatest increases in BMI by the 10-year follow-up.
Discussion
(5) Observational studies alone cannot establish a causal relationship between dieting and weight gain.
However, longitudinal follow-up studies and twin studies suggest that dieting itself may contribute to subsequent weight gain. In particular, people who engage in unhealthy weight-control behaviors have repeatedly been reported to experience significantly greater subsequent weight gain.
Conclusion
(6) Not all dieting leads to weight gain. However, unhealthy weight-control behaviors adopted by some individuals may increase the risk of subsequent weight gain.
(7) Recent research has shown that severe dietary restriction accompanied by substantial weight loss can trigger biological starvation responses involving changes in metabolism, hormones, and the nervous system. These responses may contribute to weight regain after weight loss and, in some individuals, even to weight gain beyond the pre-weight-loss level.
In addition, unhealthy weight-control behaviors may promote intestinal starvation, which could lead to an upward shift in the body-weight set point.
【 Full Text 】
-
Contents
-
- Recent background on dieting and obesity
- Issues and points to consider in observational studies
- Does dieting lead to weight gain?
- Conclusion
Introduction
In recent years, the number of people dieting for weight loss has been increasing worldwide. However, some have raised concerns that dieting itself may be accelerating the rise in obesity.
For example, some female actors and television announcers appear to have gained weight compared to the past. However, it is unlikely that they are habitually overeating; rather, they may be restricting their food intake in an effort to manage their weight.
In this article, I would like to explore whether the spread of dieting may be related to the rise in obesity, based on findings from observational and intervention studies.
1. Recent background on dieting and obesity
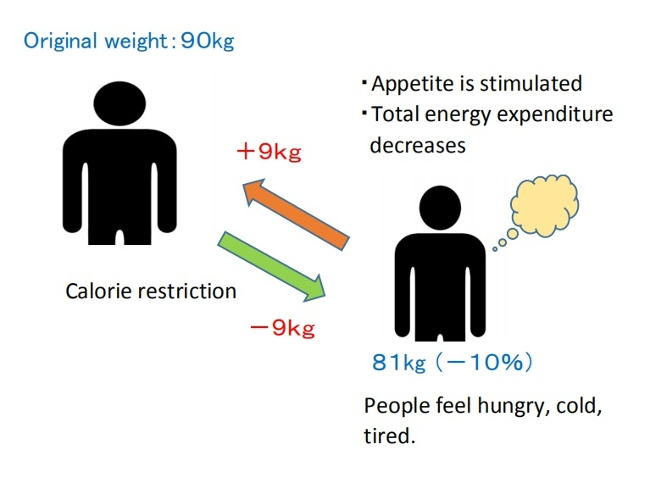
(1) In 1992, a panel of experts convened by the U.S. National Institutes of Health concluded that, with continued participation in weight-loss programs conducted in controlled settings, participants typically lose about 10% of their body weight.
However, within one year after weight loss, one-third to two-thirds of the lost weight is regained, and within five years, almost all of it is regained [1].
Studies on long-term outcomes have also shown that at least one-third of dieters regain more weight than they lost [2]. This has raised concerns that dieting may, paradoxically, produce outcomes that are directly opposite to its original purpose [2,3].
(2) The 1983 book “Dieting Makes You Fat” proposed the idea that dieting to lose weight is counterproductive for weight control because people may regain more fat than they lose with each cycle of weight loss and regain [4]. Since then, whether dieting contributes to long-term weight gain remains a controversial and actively debated topic among scientists [5,6,7].
(3) As of 1998, Americans spent over $33 billion annually on diet-related products and services [8]. Nevertheless, the prevalence of obesity has steadily increased from 30.5% (2000) to 35.7% (2010) and 42.4% (2018) [9].
The prevalence of dieting has also increased over the past several decades, paralleling the rise in the prevalence of overweight and obesity (see Table 1) [10].

Table 1: Trends in the prevalence of dieting in the U.S.
・A cross-sectional survey conducted in England (1997-2013) found that the proportion of people attempting to lose weight increased from 39% (1997) to 47% (2013).
Across all BMI categories, the proportion of individuals attempting to lose weight showed an upward trend throughout the study period [15].
Table 2 shows the 2013 figures by BMI category.
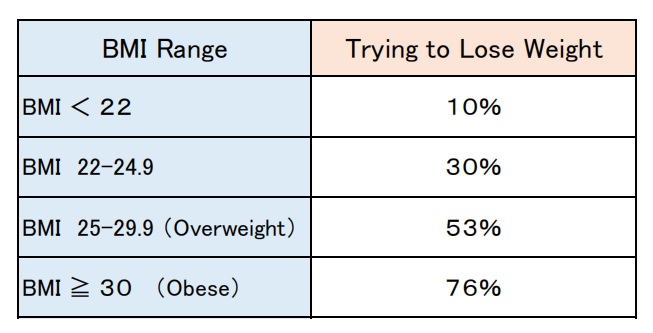
Table 2: Prevalence of weight loss attempts (2013,UK)
(4) Thus, the proportion of people attempting to lose weight has increased alongside the rising prevalence of overweight and obesity. However, this observation alone does not establish a causal relationship between the two.
Some researchers have suggested that the association between dieting and weight gain is, at least in part, causal [16,17]. Others, however, have argued that dieting is merely a proxy marker for individuals who are already prone to weight gain, and that without dieting, they would likely have gained even more weight [18].
(5) Several prospective studies have suggested that dieting is a strong predictor of future weight gain among adolescents [17,19,20], middle-aged women [21], and even individuals who were initially of normal weight [5,21,22].
・A 10-year prospective study conducted in Minnesota (1998–2009) followed 1,902 adolescents (819 males and 1,083 females) and assessed dieting status and changes in BMI at five-year intervals.
The study found that both boys and girls who reported dieting or unhealthy weight-control behaviors (Note 1) at both baseline and the 5-year follow-up experienced greater increases in BMI by the 10-year follow-up than those who did not diet [17].

Photo Credit: Freepik (photo by Prostooleh)
Note 1: Unhealthy weight-control behaviors include weight-loss practices that are generally not recommended, such as fasting, skipping meals, eating very little, and using food substitutes or diet pills.
In particular, “skipping meals” and “eating very little” were the most commonly reported unhealthy weight-control behaviors and were significantly associated with greater increases in BMI in both sexes.
The use of food substitutes (e.g. powdered products or special beverages) among males and the use of diet pills among females were associated with greater subsequent increases in BMI.
Interestingly, among girls who were overweight (25 ≤ BMI < 30) at baseline, those who continued to engage in unhealthy weight-control behaviors experienced the greatest increase in BMI over the 10-year follow-up (more than 5 BMI units), whereas those who never engaged in such behaviors showed only a minimal increase in BMI [17].
In conclusion, these findings suggest that dieting and unhealthy weight-control behaviors during adolescence may contribute to long-term weight gain [17].
(6) In 2003, an analysis of data from the 1998 National Health Interview Survey described the prevalence of specific weight-loss practices among U.S. adults (see Table 3).
Among those attempting to lose weight, only one-third reported reducing their caloric intake while increasing their physical activity [23].
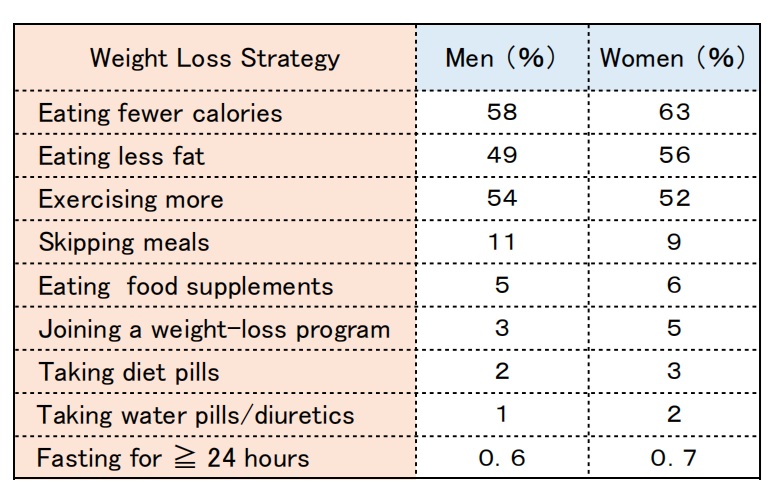
Table 3: The prevalence of weight loss strategies among U.S. adults (1998)
2. Issues and points to consider in observational studies
Previous observational studies on dieting and subsequent weight change have yielded inconsistent findings [22].
Many longitudinal observational studies have reported subsequent weight gain among self-reported dieters [17,20,21,22]. On the other hand, some studies have also reported that dieting predicts both weight loss and weight gain [24,25]. Several factors may help explain these differences in the findings.
(1) What type of dieting was followed ?
Many studies have examined whether participants were dieting at baseline, or had a history of dieting. However, relatively few have investigated the specific methods used for weight loss [21,22,26].
In addition, the terms “dieting” and “weight-loss attempts” are somewhat ambiguous and may be interpreted differently by different individuals [17].
People who adopt healthy eating and exercise habits—for example, eating more natural foods such as vegetables, reducing ultra-processed foods, eating breakfast, and exercising regularly—may be able to achieve and maintain weight loss.
In contrast, those who engage in unhealthy weight-control behaviors, such as skipping meals, eating very little, or using food substitutes (e.g. diet shakes or nutritional drinks), may experience only temporary weight loss, fail to maintain it over the long term, and eventually regain the weight.
(2) Study duration and the timing of dieting
The duration of follow-up and the timing of dieting may also influence whether long-term weight change can be evaluated accurately.
Several studies have assessed changes in body weight or BMI several years later (e.g. 2, 5, or 10 years) based on participants' dieting status at baseline [20,21,22,26].
However, people who repeatedly go on and off diets are more likely to experience substantial fluctuations in body weight.
From the perspective of body-weight homeostasis, as described by the body-weight set-point theory, individuals who were dieting at baseline may have been temporarily below their natural body weight (set point). Simply discontinuing the diet could therefore lead to subsequent weight gain.
Conversely, individuals who began dieting shortly before the end of the follow-up period may have experienced substantial weight loss because of the temporary effects of dieting.
Furthermore, when the follow-up period is as long as five or ten years, weight-control behaviors that were started or discontinued during that interval may not have been captured.
*Although not discussed here, observational studies also require caution regarding the limitations of self-reported data and the influence of confounding factors that may contribute to weight gain.
Moreover, in studies of adolescents, the natural increases in muscle mass and body weight that occur during growth should also be taken into account.
3. Does dieting lead to weight gain?
In conclusion, observational studies alone cannot establish a causal relationship between dieting and an increased risk of weight gain. However, for the following reasons, I believe that dieting is likely to contribute to weight gain.
(1) Is dieting merely a proxy marker?
One interpretation is that dieting is simply a proxy marker reflecting the global trend toward increasing body weight, rather than a cause of weight gain itself. From this perspective, it is argued that without dieting, people would gain even more weight [18].
However, the 10-year study of adolescents discussed in Section 1(5) made it possible to compare the weight trajectories of participants who were dieting at baseline but had stopped dieting five years later with those who continued dieting.
The researchers found that those who stopped dieting gained substantially less weight than those who continued dieting. Based on these findings, they did not support the claim that people would gain even more weight if they did not diet [17].
(2) Are people with a genetic predisposition to obesity more likely to diet?
Another explanation for the association regarding dieting and obesity is that dieting itself does not cause subsequent weight gain. Rather, people who are genetically prone to obesity may simply be more likely to go on a diet [6].
However, the 10-year study of adolescents yielded findings that were not consistent with this claim.
Among girls who were already overweight at baseline, those who continued to engage in unhealthy weight-control behaviors showed significantly greater increases in BMI than those who had never engaged in such behaviors. The researchers suggested that dieting itself may contribute to subsequent weight gain [17].
Furthermore, a longitudinal twin study conducted in Finland examined changes in body weight among twins with different numbers of intentional weight-loss episodes of at least five kg.
Although the study could not rule out the influence of genetic and shared family factors on weight gain, it also suggested that dieting itself may contribute to subsequent weight gain [16].
(3) Mechanisms that promote weight rebound after weight loss
Recent research has greatly improved our understanding of energy homeostasis and the mechanisms that regulate body weight.
Severe dietary restriction accompanied by substantial weight loss can trigger biological starvation responses involving changes in metabolism, hormones, and the nervous system, potentially leading to increased appetite and overeating. As a result, body weight tends to return toward its previous level and may even exceed the pre-weight-loss level in some individuals [27,28].
In addition, fasting for weight control (going without food for 24 hours) has been suggested to be associated with a greater risk of developing binge-eating disorder in the future than less severe dieting behaviors [29].
Furthermore, an overshoot in body weight during the recovery period has been documented in normal-weight participants in both the classic Minnesota Starvation Experiment and the U.S. Army Ranger multistressor study [30,31].
(4) A possible link to intestinal starvation
My intestinal starvation theory suggests that when all ingested food has been completely digested within the intestinal tract, the body may perceive this as a state in which no food is present. This may be described as a modern form of hunger that can occur even in affluent societies—a condition that may have become more likely with advances in food processing and the spread of ultra-processed foods.
Calorie-restricted dieting, especially unhealthy weight-control behaviors such as skipping meals, eating very little, or using food substitutes instead of regular meals, may further promote this intestinal starvation.
4. Conclusion
Not all dieting leads to weight gain. Some people successfully lose weight and maintain their weight loss by adopting healthy dietary patterns and regular physical activity.
In fact, adherence to the Mediterranean diet has been reported to be inversely associated with the risk of overweight, obesity, and long-term weight gain [32].

Photo Credit: Freepik (Photo by Katemangostar)
In contrast, people who adopt unhealthy weight-loss strategies—such as fasting, skipping meals, eating very little, or using food substitutes—have repeatedly been reported to experience significantly greater subsequent weight gain than those who do not diet or who follow healthy weight-loss strategies [17,33].
These approaches may therefore lead to outcomes that are contrary to their original purpose.
Recent research has shown that severe dietary restriction accompanied by substantial weight loss can trigger biological starvation responses involving changes in metabolism, hormones, and the nervous system [27,28,34]. These changes may help explain why body weight often returns after weight loss and, in some cases, even exceeds the pre-weight-loss level.
In addition to these biological responses, I believe that unhealthy weight-control behaviors, particularly dietary restriction, are also likely to promote intestinal starvation, thereby contributing to an upward shift in the body-weight set point.
<References>
[1] Methods for voluntary weight loss and control. NIH Technology Assessment Conference Panel. Ann Intern Med. 1992 Jun 1;116(11):942-9.
[2] Mann T et al. Medicare's search for effective obesity treatments: diets are not the answer. Am Psychol. 2007 Apr;62(3):220-33.
[3] Bacon L, Aphramor L. Weight science: evaluating the evidence for a paradigm shift. Nutr J. 2011 Jan 24;10:9.
[4]Cannon G, Einzig H. Dieting makes you fat. London: Century Publishing; 1983.
[5] Jacquet P et al. How dieting might make some fatter: modeling weight cycling toward obesity from a perspective of body composition autoregulation. Int J Obes (Lond). 2020 Jun;44(6):1243-1253.
[6] Hill AJ. Does dieting make you fat. Br J Nutr. 2004 Aug;92 Suppl 1:S15-8.
[7] Lowe MR. Dieting: proxy or cause of future weight gain? Obes Rev. 2015 Feb;16 Suppl 1:19-24.
[8] Cleland R et al. Commercial weight loss products and programs: what consumers stand to gain and lose. Crit Rev Food Sci Nutr. 2001 Jan;41(1):45-70.
[9] National Center for Health Statistics, National Health and Nutrition Examination Survey, 1999–2018.
[10] Montani JP et al. Dieting and weight cycling as risk factors for cardiometabolic diseases: who is really at risk? Obes Rev. 2015 Feb;16 Suppl 1:7-18.
[11] Williamson DF et al. Weight loss attempts in adults: goals, duration, and rate of weight loss. Am J Public Health. 1992 Sep;82(9):1251-7.
[12]Serdula MK et al. Prevalence of attempting weight loss and strategies for controlling weight. JAMA. 1999 Oct 13;282(14):1353-8.
[13] Weiss EC et al. Weight-control practices among U.S. adults, 2001-2002. Am J Prev Med. 2006 Jul;31(1):18-24.
[14] Yaemsiri S et al. Perceived weight status, overweight diagnosis, and weight control among US adults: the NHANES 2003-2008 Study. Int J Obes (Lond). 2011 Aug;35(8):1063-70.
[15] Piernas C et al. Recent trends in weight loss attempts: repeated cross-sectional analyses from the health survey for England. Int J Obes (Lond). 2016 Nov;40(11):1754-1759.
[16]Pietiläinen KH et al. Does dieting make you fat? A twin study. Int J Obes (Lond). 2012 Mar;36(3):456-64.
[17] Neumark-Sztainer D et al. Dieting and unhealthy weight control behaviors during adolescence: associations with 10-year changes in body mass index. J Adolesc Health. 2012 Jan;50(1):80-6.
[18] Stice E, Presnell K. Dieting and the eating disorders. In: Agras WS, editor. The Oxford Handbook of Eating Disorders. Oxford University Press; USA: 2010. pp. 148–179.
[19] Neumark-Sztainer D et al. Why does dieting predict weight gain in adolescents? : a 5-year longitudinal study. J Am Diet Assoc. 2007 Mar;107(3):448-55.
[20]Viner RM, Cole TJ. Who changes body mass between adolescence and adulthood? Factors predicting change in BMI:1970 British Birth Cohort. Int J Obes (Lond). 2006 Sep;30(9):1368-74.
[21]Korkeila M et al. Weight-loss attempts and risk of major weight gain: a prospective study in Finnish adults. Am J Clin Nutr. 1999 Dec;70(6):965-75.
[22] Sares-Jäske L et al. Self-report dieting and long-term changes in body mass index and waist circumference. Obes Sci Pract. 2019 Mar 26;5(4):291-303.
[23] Kruger J et al. Attempting to lose weight: specific practices among U.S. adults. Am J Prev Med. 2004 Jun;26(5):402-6.
[24] Bild DE et al. Correlates and predictors of weight loss in young adults: the CARDIA study. Int J Obes Relat Metab Disord. 1996 Jan;20(1):47-55. PMID: 8788322.
[25] Coakley EH et al. Predictors of weight change in men: results from the Health Professionals Follow-up Study. Int J Obes Relat Metab Disord. 1998 Feb;22(2):89-96.
[26] French SA et al. Predictors of weight change over two years among a population of working adults: the Healthy Worker Project. Int J Obes Relat Metab Disord. 1994 Mar;18(3):145-54. PMID: 8186811.
[27]Maclean PS et al. Biology's response to dieting: the impetus for weight regain. Am J Physiol Regul Integr Comp Physiol. 2011 Sep;301(3):R581-600.
[28]Ochner CN et al. Biological mechanisms that promote weight regain following weight loss in obese humans. Physiol Behav. 2013 Aug 15;120:106-13.
[29]Stice E et al. Fasting increases risk for onset of binge eating and bulimic pathology: a 5-year prospective study. J Abnorm Psychol. 2008 Nov;117(4):941-6.
[30] Keys, A, Brozek, J, Henschel, A et al. (1950) The Biology of Human Starvation. Minnesota: University of Minnesota Press.
[31] Nindl BC et al. (1997) Physical performance and metabolic recovery among lean, healthy men following a prolonged energy deficit. Int J Sports Med 18, 317–324.
[32] Lotfi K et al. Adherence to the Mediterranean Diet, Five-Year Weight Change, and Risk of Overweight and Obesity: A Systematic Review. Adv Nutr. 2022 Feb 1;13(1):152-166.
[33]Savage JS, Birch LL. Patterns of weight control strategies predict differences in women's 4-year weight gain. Obesity (Silver Spring). 2010 Mar;18(3):513-20.
[34] Mann T et al. Promoting Public Health in the Context of the "Obesity Epidemic": False Starts and Promising New Directions. Perspect Psychol Sci. 2015 Nov;10(6):706-10.
2022.11.11
Why Are Sumo Wrestlers So Fat?; Six Reasons They’ve Adapted to the Gut Starvation Mechanism
Contents
<Introduction>
- The same mechanism as people who rebound after dieting
- The six reasons that I believe it is a starvation mechanism
<The bottom line>
<Introduction>
Have you ever seen a sumo wrestler right in front of you? When I was working as a waiter at a hotel several years ago, there was a pep rally for sumo wrestlers, and I was able to see them up close.
Also, at the 2017 Osaka tournament in Japan, I observed the morning practice of a team and was allowed to sample their breakfast called "chanko."

I had a sample of "chanko."
I got the impression that they are big-boned, with steel-like muscles, and a lot of body fat on top of that.
Their average body fat percentage is said to be around thirty percent or more, but there are some wrestlers in the twenty percent range, not that different from the average person. They are like a mass of muscles.
It is generally believed in Japan that wrestlers will gain weight because they eat a lot and sleep well including taking naps, but I can explain that they have successfully adopted the mechanism of intestinal starvation.
1. The same mechanism as people who rebound after dieting
In Japan, the image of sumo wrestlers in particular may lead to the image that "eating more makes you fat," but I would like to explain that this is the same mechanism as "those who end up rebounding after dieting and gain more weight than before" or "those who gradually gain weight by skipping breakfast or having a late dinner.”
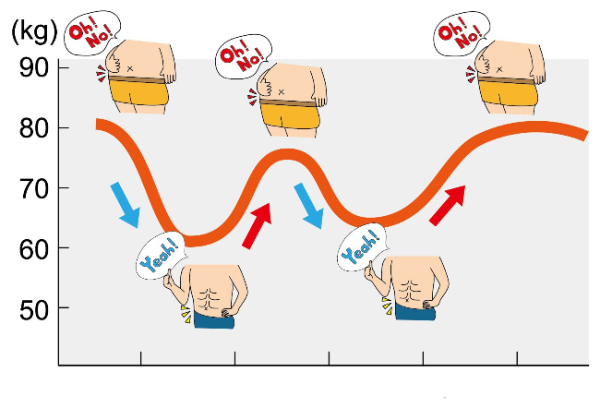
First of all, I'm going to illustrate how both of them gain weight in the figure below.
■The concept of a person who gains more weight than before after dieting
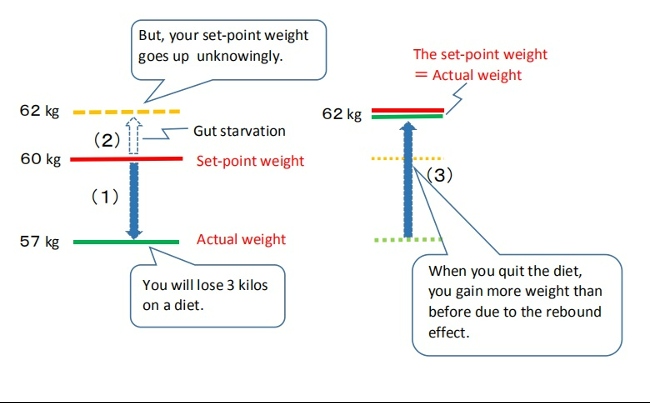
(1)→ (2)→ (3)
(1) You will lose a little weight through caloric restriction or exercising, etc.
(2) When you eat less (especially with an unbalanced diet), and you feel hungry for an extended period of time, you tend to starve your gut, and your set-point for body weight may go up without you realizing it.
(3) Later, when you start eating as you did before dieting, your weight will be higher than before.
■The concept of sumo wrestlers gaining weight
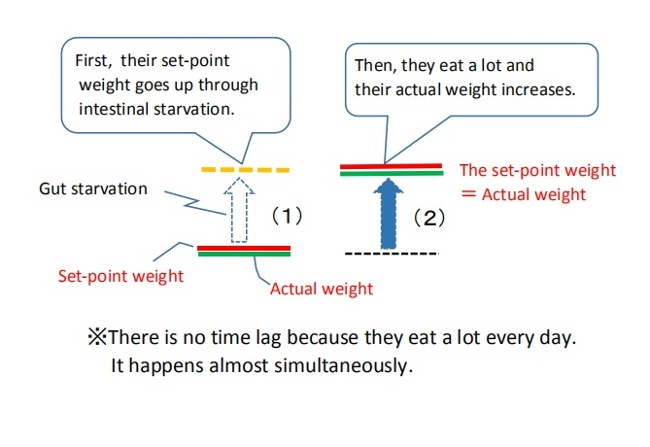
(1) → (2)
(1)First, by their traditional unique diet and hard practice, intestinal starvation can be induced. Their set-point weight goes up.
(2)Then, they eat a lot and thire actual weight increases (weight gain).
If you are a dieter, there is a time lag, but in the case of wrestlers, they eat good amounts of food every day, so it happens almost simultaneously.
Although they appear to eat a lot and are gaining weight, if intestinal starvation is not induced, their weight should not increase as much as expected.
2. The six reasons that I believe it is a starvation mechanism
When you see big eaters in a food eating competition, some may ask, "Why don't they get fat even though they eat so much?” But, from my theory, it is not at all surprising.
It’s not that they have a special "non-fattening constitution," but that anyone who eats like that from morning to night is less likely to gain weight (although I wonder why they can eat so much food at once).
Please understand that the way of eating of a sumo wrestler is a far cry from that of an eating competitor.
■An explanation of why the way of eating and exercising of sumo wrestlers can easily induce intestinal starvation. (1) - (6)
(1)A wrestler must weigh at least sixty-seven kilograms to be admitted. People who are overweight or muscular from the beginning tend to have stronger stomachs, and are thought to have a relatively high digestive rate. Such people are more likely to induce gut starvation than thin people.

(2) The basic diet for sumo wrestlers is called "chanko," which consists of easily digestible proteins such as chicken, fish, tofu, etc., and vegetables, slowly simmered in soy sauce. It is relatively low in fat and easy to digest.
(3) Sumo wrestlers generally eat a good amount of rice. By eating a lot of rice and soup, the stomach expands (the balloon effect), which leads to creating the dilution effect and push-out effect of food in the stomach.
[Related article]
(4)They traditionally eat two meals a day: the first meal is around eleven a.m. after morning practice, and dinner is around six p.m.
Since they practice from the early morning without breakfast, if dinner is finished at seven p.m., it means that they do not eat for about fifteen to sixteen hours until the next meal. It make sense to do intense morning training on an empty stomach to gain weight.
Of course, there are some wrestlers who try to eat snacks or supplements late at night in order to take in more calories, but my idea is that it makes easier to gain weight when they don't eat.

(5)Strength training is a force for gaining strength, and it ultimately works in the direction of weight gain. Eating two meals a day and exercising intensely will make sumo wrestlers gain more weight.
(6)Most of the food in the pot is eaten first by the top-ranked wrestlers. The lower-ranked wrestlers eat next, and lastly the new trainees.
The last people have to eat a big ball of rice and leftovers, which consists of only a little meat and most of the soup.
However, it is said that this kind of meal tends to make sumo wrestlers gain more weight.
The bottom line
(1)Sumo wrestlers are famous for being big and fat, but they do not gain weight because their daily caloric intake exceeds their daily caloric expenditure.
Their traditional diet and exercise makes sense in terms of weight gain in that it facilitates the creation of intestinal starvation.
(2)Intestinal starvation is more likely to be induced when a person who has a big body from the start eats relatively easily digestible foods with lots of carbohydrates (rice) and two meals a day.
(3)The mechanism by which wrestlers gain weight is the same as that of "people who diet and gain more weight than before due to the rebound effect.”
In the case of sumo wrestlers, since they eat a lot every day, this happens almost simultaneously, and they appear to eat a lot and gain weight.
2019.11.21
Weight Loss Without Rebounding Requires Two Steps
Summary
(1)Just as weight gain does, weight loss likely involves two distinct physiological processes. Under conventional calorie restriction, the body tends to perceive an energy deficit and triggers adaptive responses aimed at maintaining the previous body weight level. As a result, weight loss is difficult to sustain, and body weight often returns to its original range.
To achieve long-term weight loss without rebounding, it is necessary to lower the body’s weight “set-point” itself.
(2)Lowering this set-point likely requires at least two physiological steps.
First, before reducing body weight, it is essential to establish a physiological environment in which the body does not perceive energy deprivation. Second, within that environment, undergo a process where body fat naturally decreases over time.
Step One:
The diet is structured around foods that are nutrient-dense and slow-digesting, such as vegetables, dairy products, nuts, and certain protein-rich foods.
When intestinal contents containing less digestible matter remain in the gut for extended periods, this may be perceived by the body as a signal that food is sufficiently available. As a result, even if overall energy balance becomes slightly negative, strong adaptive responses are less likely to be triggered.
Step Two :
Sustained satiety not only helps prevent overeating, but may also gradually reduce absorption efficiency. Over the long term, coordinated interactions between the brain—particularly the hypothalamus—and peripheral organs and tissues may allow body fat to decline in a stepwise manner.
(3)Although the two-step approach may result in a dietary pattern that resembles a low-carb diet, the underlying goal is fundamentally different.
Low-carb diets primarily aim to reduce insulin secretion by restricting carbohydrate intake. In contrast, the two-step approach focuses on creating a physiological environment opposite to intestinal starvation. To achieve this, it reduces carbohydrate intake while increasing the intake of nutrient-dense foods that take longer to digest, in sufficient amounts.
【Full text】
-
Contents
-
- Two distinct physiological processes underlying weight loss
- What is required to lower the set-point for body weight?
Step one
Step two - How the two-step approach differs from low-carb diets
Although this blog is not intended as a diet guide, examining the mechanisms of weight gain inevitably requires me to also organize, in theoretical terms, the opposite process—how people lose weight.
In this article, I will outline a theory of sustainable weight loss based on my own hypothesis. This discussion is theoretical rather than practice-based, and its purpose is to share a new way of thinking free from conventional constraints.
1. Two distinct physiological processes underlying weight loss
I propose that just as weight gain involves two physiologically distinct processes, weight loss can also occur through two physiologically distinct processes.
(1) Weight decreases, but rebounds
Conventional calorie restriction and low-fat diets are designed to reduce body weight by decreasing energy intake and increasing energy expenditure. This approach often involves constant hunger.
In this blog, I use the body weight set-point hypothesis[1,2] as a framework to explain weight homeostasis.
When energy intake is severely restricted and body weight decreases, the body perceives an energy deficit and triggers adaptive responses aimed at preserving stored energy[3,4].
These responses are best understood as adaptive processes that consist of interacting changes in metabolism, neuroendocrine function, autonomic regulation, and behavior[5].
In addition, in my opinion, prolonged hunger leads the body to extract as much nutrition as possible from food, thereby increasing absorption efficiency.
In most cases, however, the body’s weight set-point itself does not change. As a result, weight loss is not sustained, and body weight is likely to return to its original range over time.
【Related article】
Biological Responses Driving Weight Rebound After Weight Loss
(2) Lowering the body weight “set-point” itself
I believe that the fundamental problem in obesity lies in an elevated body weight set-point.
Even though obese individuals have ample energy stores, they still exhibit metabolic resistance to caloric restriction, suggesting that obesity represents a physiologically stable state for some people[1]. Animal studies similarly describe obesity as a condition of energy homeostasis regulated around a higher set-point[1].
Therefore, achieving long-term weight loss requires not merely focusing on short-term energy balance, but lowering the body weight set-point itself. Relevant literature supporting this perspective is cited below.
"There appears to be a “set point” for body weight and fatness, and the problem in obesity is that the set point is too high.(*snip*)
There are two prominent findings from all the dietary studies done over the years.
First: all diets work. Second: all diets fail.
What do I mean?
Weight loss follows the same basic curve so familiar to dieters. Whether it is the Mediterranean, the Atkins or even the old fashioned low-fat, low-calorie, all diets in the short term seem to produce weight loss. Sure, they differ by amount lost–some a little more, some a little less. But they all seem to work.
However, by six to twelve months, weight loss plateaus, followed by a relentless regain, despite continued dietary compliance.(*snip*)
So all diets fail. The question is why.
Permanent weight loss is actually a two-step process. There is a short-term and a long-term (or time-dependent) problem. "
( Fung J. 2016. The obesity code. pages 62,215 )
2. What is required to lower the set-point for body weight?
In my understanding, the “two-step process” described by Doctor Fung is a conceptual framework that views obesity treatment (weight loss) as consisting of a short-term and a long-term challenge, organized primarily from a clinical and practical perspective.
On the other hand, this article focuses on the long-term problem—specifically, why the body resists weight loss and why body weight,once reduced, often returns over time[6]—and explores this issue more deeply from a physiological perspective.
Based on this analysis, I suggest that successful long-term weight loss requires at least the following two physiological steps:
(1) Before trying to lose weight, creating a physiological state in which the body does not perceive energy deprivation.
(2) Within that state, allowing body fat to decrease naturally over time.
My theory posits that weight gain accompanied by an upward shift in the body’s set-point weight is closely related to adaptive responses that arise when the body perceives a state of starvation. Therefore, I believe that reducing body weight in a sustained manner require creating the opposite physiological environment.
Many diets aim for losing weight from the very beginning. However, when the first step is skipped, the body tends to activate adaptive responses to restore homeostasis[6], which can increase the likelihood of long-term weight rebound.
Specifically, the process can be described as follows.
Step one
Rather than reducing overall food intake and enduring hunger, this approach centers the diet around nutrient-dense foods that either take longer to digest or are partially indigestible.
More specifically, this involves reducing the intake of refined carbohydrates and instead increasing consumption of foods such as whole grains, fiber-rich vegetables, nuts, dairy products, fat, and minimally processed protein foods.

Author: brgfx. Source: Freepik
As a result, intestinal contents that include less easily digestible matter remain in the gut for a longer period of time. This may not only reduce the sensation of hunger but also may be perceived by the body as a signal that food is sufficiently available. Consequently, even if overall energy balance becomes slightly negative, the body is less likely to perceive this state as energy deprivation.
Step two
As hunger diminishes, appetite tends to decrease, and absorption efficiency may also gradually decline. Eventually, I suggest that coordinated interactions between the brain—centered on the hypothalamus—and peripheral organs and tissues[7] may contribute to a gradual reduction in body fat.
Changes in absorption efficiency may not be intuitive at first glance, but consider this: consuming carbohydrates in a state of intense hunger tends to cause a rapid rise in blood glucose levels, whereas eating them several hours after a meal moderates the rise. Similarly, alcohol intoxication occurs faster on an empty stomach, but more gradually after eating.
Thus, by avoiding prolonged hunger and consuming foods that require longer digestion at appropriate intervals, absorption efficiency may gradually decrease in relative terms.
3. How the two-step approach differs from low-carb diets
The “two-step approach” proposed here may, in practice, result in a dietary pattern that resembles a low-carbohydrate diet. However, the two differ fundamentally in their starting points and underlying goals. In this section, I will clarify these differences.
▽Low-carb diets primarily aim to limit carbohydrate intake in order to suppress rapid spikes in blood glucose and reduce insulin secretion, which plays a key role in fat storage.
When energy derived from carbohydrates becomes insufficient, the body shifts to using fat as its main energy source, entering what is known as a state of ketosis. As a result, body fat tends to be utilized more readily, and body weight may decrease relatively quickly.
Another commonly cited feature of low-carb diets is that they do not require strict calorie counting, and often promote satiety through higher protein and fat intake.
▽In contrast, my own theory likewise considers diets heavily skewed toward refined carbohydrates and highly processed foods to be likely contributors to the modern obesity epidemic. However, this is not because carbohydrates themselves are inherently harmful in a direct sense.
What I emphasize instead are certain properties of carbohydrates: their rapid digestibility; the “dilution effect” that occurs when carbohydrates are consumed together with large amounts of water; and the “push-out effect,” whereby gastric contents are rapidly propelled into the intestine.
Author: brgfx. Source: Freepik
When these factors act together, all ingested food may be digested and expelled relatively quickly, potentially increasing the likelihood of intestinal starvation under specific conditions.
【Related article】
The Dilution Effect/ Pushing Out Effect of Carbohydrates
For this reason, the two-step approach aims to create a physiological environment opposite to intestinal starvation—namely, a state in which intestinal contents containing less digestible matter remain in the gut for an extended period. To achieve this, carbohydrate intake is reduced in order to weaken the dilution and push-out effects, while the relative intake of other foods—such as fiber-rich vegetables, dairy products, fats, and minimally processed protein sources—is increased.
In low-carb diets, by contrast, the central strategy is to reduce carbohydrate intake itself, while proteins and fats are consumed relatively freely as alternative energy sources. This distinction represents a fundamental difference between low-carb diets and the two-step approach described here.
References
[1]Richard E. Keesey, Matt D. Hirvonen, Body Weight Set-Points: Determination and Adjustment, The Journal of Nutrition, Volume 127, Issue 9, 1997, Pages 1875S-1883S, ISSN 0022-3166.
[2]Ganipisetti VM, Bollimunta P. Obesity and Set-Point Theory. 2023 Apr 25. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–.
[3]Hall KD, Guo J. Obesity Energetics: Body Weight Regulation and the Effects of Diet Composition. Gastroenterology. 2017 May;152(7):1718-1727.e3.
[4]Egan AM, Collins AL. Dynamic changes in energy expenditure in response to underfeeding: a review. Proc Nutr Soc. 2022 May;81(2):199-212.
[5] Rosenbaum M, Leibel RL. Adaptive thermogenesis in humans. Int J Obes (Lond). 2010 Oct;34 Suppl 1(0 1):S47-55.
[6] Ochner CN et al. Biological mechanisms that promote weight regain following weight loss in obese humans. Physiol Behav. 2013 Aug 15;120:106-13.
[7] Wilson JL, Enriori PJ. A talk between fat tissue, gut, pancreas and brain to control body weight. Mol Cell Endocrinol. 2015 Dec 15;418 Pt 2:108-19.
2018.05.30
Why Do We Gain Weight even Though We Eat Small Portions of Food?
Contents
- A woman friend who eventually put on some weight
- A colleague who gained three kilograms in a year
- "Just reduce calories" is a mistake
It is said that the cause of weight gain is the caloric intake exceeding calories burned through metabolism and activity. For this reason, I see people dieting by only reducing the amount of food they eat, and putting up with being hungry over long hours.

For example, they eat only a rice ball and a piece of fried chicken, or a hamburger and a drink for lunch. These people say they are hungry but continue experiencing hunger for long periods of time.
In my opinion, people like this not only do not diet well, but they also tend to gain weight eventually.
1. A woman friend who eventually put on some weight
When I was working part-time at a restaurant in college, there was a woman who wasn’t that overweight, but she started dieting anyway.
She wasn’t slim, but she wasn’t overweight, either. To me, she looked healthy and fit. I thought she was okay as she was. But it seemed that she started dieting because she wanted to get slim.

Therefore, she only ate half of her meal, such as rice and meat/fish dish and never any vegetables. She was always saying, “I’m starving...” but continued experiencing hunger and stopped eating snacks.
As a result, not only did she not lose weight, but she also gained a little weight.
2. A colleague who gained three kilograms in a year
The same goes for my colleague, T, who worked as a cook in the kitchen at a nursing home. When I first met him, he was a stocky guy (about 170cm tall and 70 kilos).
He wasn’t overweight but he was on a diet, saying he had gained three kilos which shattered his previous weight level in the last year.

In his case, he was working before six a.m., but he hardly ever ate breakfast.
For lunch, he only ate a small bowl of rice and meat or fish. He almost never ate vegetable dishes such as salad and simmered vegetables (traditional Japanese vegetable stew).
He gained two more kilos in the following year.
3. "Just reduce calories" is a mistake
What's wrong with this is, that the people previously mentioned thought that in order to lose weight, they only needed to reduce calories from carbohydrates, meat, and fat, etc. Furthermore, they thought they had to be hungry in order to lose weight.
As a result, I can posit that intestinal starvation was induced because they didn’t consume fiber from vegetables, fat, and dairy products, etc. very much, causing the set-point weight to increase.

There are two ways in which the intestinal starvation mechanism occurs.
(1) Eating regular or big portions of an unbalanced meal, but not eating as often (e.g. skipping breakfast and eating two meals a day) and experiencing hunger over many hours.
(2)Eating small portions as seen in dieters or pregnant women, sometimes skewed towards digestible carbohydrates and protein, etc. Even if they eat three times a day, they often experience hunger over many hours.
In conclusion, whether you eat a good amount of food or a small portion of food, if your diet consists of mostly digestible carbs and some protein, an imbalance of food in the intestines remains the same. If you don’t eat anything else and experience hunger over many hours, it leads to the similar effect in view of creating intestinal starvation.
Eating vegetable dishes, dairy products and fat/oil, etc. is important with regards to preventing intestinal starvation, but those people in the previous examples were only conscious of caloric intake, and chose not to eat them.
2017.12.07
After Gaining Weight, We Eat Too Much and Do Less Exercise
-
Contents
-
<Prologue>
- Rats don’t get fat from eating too much
- Example of not enough exercise after getting fat
Prologue
"The experts who say that we get fat because we overeat or we get fat as a result of overeating - the vast majority - are making the kind of mistake that would (or at least should) earn a failing grade in a high-school science class.
They're taking a law of nature that says absolutely nothing about why we get fat and a phenomenon that has to happen if we do get fat - overeating - and assuming these say all that needs to be said."
(Gary Taubes. 2011. Why we get fat. New York: Anchor Books, Page 76.)

This is the foundation I started writing my blog on. I’m sure that there are at least a few researchers in the world who think the same way as I do.
Even if someone insisted that, “the Earth is going around the Sun” in the sixteenth or seventeenth century where "geocentric theory" was the prevailing thought, no one would have believed him.
Many should have argued that, “if the Earth is going around the sun, our heads should go around, too.” However, now, it’s common sense that the Earth is going around the sun.
In the same way, many might not believe me when I say, “people can gain weight by intestinal starvation and it is the fundamental cause of being overweight.” However, I believe it’s the truth.
1.Rats don’t get fat from eating too much
It is said that, “eating too much and not enough exercise are the causes of gaining weight,” but here is an interesting experiment that is related to it.
"In the early 1970s, a young researcher at the University of Massachusetts named George Wade set out to study the relationship between sex hormones, weight, and appetite by removing the ovaries from rats (females,obviously) and then monitoring their subsequent weight and behavior.
The effects of the surgery were suitably dramatic: the rats would begin to eat voraciously and quickly become obese.The rat eats too much, the excess calories find their way to the fat tissue, and the animal becomes obese. This would confirm our preconception that overeating is responsible for obesity in humans as well.

But Wade did a revealing second experiment, removing the ovaries from the rats and putting them on a strict postsurgical diet. (*snip*) The rats, postsurgery, were only allowed the same amount of food they would have eaten had they never had the surgery.
What happened is not what you'd probably think. The rats got just as fat, just as quickly. But these rats were now completely sedentary. They moved only when movement was required to get food. (*snip*)
The way Wade explained it to me, the animal doesn't get fat because it overeats, it overeats because it's getting fat. The cause and effect are reversed.
(*snip*)
The evidence that fat tissue is carefully regulated, not just a garbage can where we dump whatever calories we don't burn, is incontrovertible.(*snip*)
Those who get fat do so because of the way their fat happens to be regulated and that a conspicuous consequence of this regulation is to cause the eating behavior (gluttony) and the physical inactivity (sloth) that we so readily assume are the actual causes."
(Taubes. Why we get fat. Page 89-90, 93-4.)
<1970s>
Words of Bruce Birstrian who conducted a treatment of a low-calorie diet (600kcal/day) to thousands of obese patients at Harvard University of Medicine.

"Undereating isn't a treatment or cure for obesity; it's a way of temporarily reducing the most obvious symptom. And if undereating isn't a treatment or a cure , this certainly suggests that overeating is not a cause."
(Taubes. Why we get fat. Page 39.)
My experience is a little different from the rats’ story, but I want to tell of my experience that I gained weight not because of eating more.
When I was very thin, under forty kilograms, I couldn’t eat a lot since my stomach always felt heavy. Fatty foods and oily foods were the worst. I tried hard to gain weight, but I couldn’t.
One day, I realized that I could gain weight by eating only easy-to-digest foods (mainly carbs and a little meat) and experiencing being hungry for hours. So, I tried to eat light meals for breakfast and lunch, and I tried not to eat vegetables and fat very much until dinner. By doing so, I gradually gained weight. And when I weighed about fifty kilograms, I had more muscle and less discomfort in my stomach. I was able to eat more than before.
Those who didn’t know my experience told me, “You’re gaining weight because you’re eating more,” but that wasn’t true.
After my body adjusted to my new eating plan, I gained weight little by little by eating. As I gained weight, I gradually gained more muscle and my appetite increased. As a result, I was able to eat more than before. So, the reality was the other way around.
▽Maybe it’s easier for you to imagine with an extreme example.
Let’s say there is a big man who is three meters tall and weighs two-hundred-fifty kilograms. If he eats five times as much food as we do, we would not think that he has grown big because he eats so much. Rather, we would think, "He is able to eat that much because he is so big.”
"Just prior to the Second World War, European medical researchers argued that it is absurd to think about obesity as caused by overeating, because anything that makes people growーwhether in height or in weight, in muscle or in fatーwill make them overeat.
Children, for example, don't grow taller because they eat voraciously and consume more calories than they expend. They eat so muchーovereatーbecause they're growing."
(Taubes. Why we get fat. Page 9.)
2.Example of not enough exercise after getting fat

"Some people find it hard to get their head round the fact that aerobic exercise is not particularly effective for weight loss, even when faced with all the facts.
One reason for this is our experience of seeing physically fit and active individuals who are clearly lean.
Look at any elite long-distance runner or Tour de France cyclist and you're probably getting a glimpse of what it's like to have a single-digit body fat percentage. The automatic thought process is that exercise causes leanness.
However, could it that individuals who are naturally lean are simply more likely to end up as elite long-distance runners or cyclists? In other words, might their natural leanness cause certain people to be more active, rather than the other way round?
There's actually some evidence for this. In one piece of research, the relationship between physical activity and body fatness in children over a 3-year period was assessed. It was found that the more sedentary children were, the more fat they carried.

This is all to be expected, but because the study was conducted over a prolonged period the researchers were able to gauge whether sedentary behaviour preceded weight gain.
Actually, it did not. In reality, children accumulated fat first, and then became more sedentary.
The authors noted that this finding 'may explain why attempts to tackle childhood obesity by promoting PA [physical activity] have been largely unsuccessful'. "
(Jone Briffa. 2013. Escape the Diet Trap. London: Fourth Estate, Pages 223-4.)
I agree with this opinion, but I’d like to add my own opinion.
As Dr. Briffa said, I think it’s reasonable to think those who are slim aim to be marathon athletes or soccer players, etc. They at least know that they can eat a lot and not get fat. So they will eat whatever they want without hesitation, won’t they?
In other words, by eating balanced foods every meal, intestinal starvation doesn’t happen —by that, I mean their set-point for body weight doesn’t change—and they keep their current weight while getting a little more muscle.
On the other hand, when people stay at home, spending time relaxing with a book or watching television, or when doing office work or light physical labor, don’t they tend to eat less or lighter meals?

Sometimes, they may eat only light meals such as hamburgers, hot-dogs, or instant noodles for lunch. Since they don’t exercise, they don’t pay attention to eating balanced and nutritious meals.
If their diet leans toward easily digestible carbs and some protein and they are experiencing being hungry for hours, the intestinal starvation mechanism may occur and their set-point weight will go up. They end up gaining more weight.
To sum up, I’d like to say that not enough exercise or laziness won’t directly cause people to get fat. The intensity and amount of physical activity will affect the amount of food you eat as well as food choices.
2017.09.28
What Does It Mean to Eat Relatively Less?
Contents
- An example of judo
- An example of delivery center
- An example of food
<The bottom line>

I always felt something was wrong, when I was having lunch with my coworker K, who is about eighty kilograms. He said to me, “You have to eat more in order to gain weight”, because I was very thin.
However, he was eating the same thing as I was. It’s just that he had a little more rice than I.
Why It felt odd was that "K was eating relatively less" and " I was eating relatively more " in terms of quality and quantity.
1. An example of "judo"
First, I’d like to explain by using the Japanese sport of judo. There are usually wrestlers of forty-five, sixty, and up to ninety kilograms mixed weight groups at a practice.
The forty-five kilogram wrestler often works with those who are heavier than him, so he will be practicing relatively hard. In particular, if he practices with a ninety kilogram wrestler, there is twice the difference of weight, so it’s difficult to win.
On the other hand, for the ninety kilogram wrestler, it’s a practice which is relatively easy, since there are only those who weigh less than him. Even if they do the same practice, the level of challenge is different for each wrestler.
2. An example of delivery center
Let’s see it again here by using a “delivery center” example. A delivery center is a place where they sort packages and send them out everyday. There are two delivery centers. Center A has a capacity of five hundred packages, and delivery center B has a capacity of eight hundred packages.
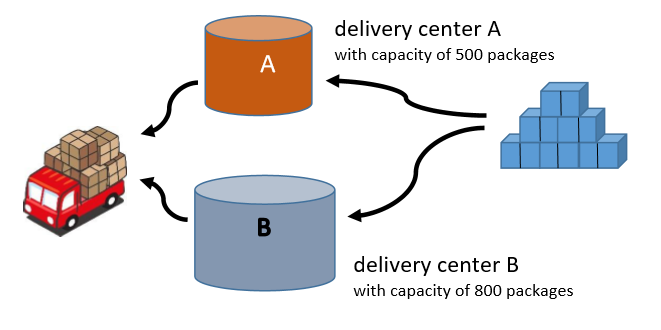
When there are five hundred packages being processed, A will be at its limit, but B still has some room.
When there are seven hundred packages being processed, A is over its capacity, so employees have to work overtime, but B still has some room.
That is to say, even if the quantity of packages is the same, the things happening inside differ by their capacity. If this were food, then the package would be equivalent to the “intake amount of food.”
3. An example of food
I guess you already know what I want to say. Here again, we have three ladies of different weights eating the same thing. A: 90kg, B: 60kg, C: 45kg.
Let’s say all three had the same hamburger set for lunch.
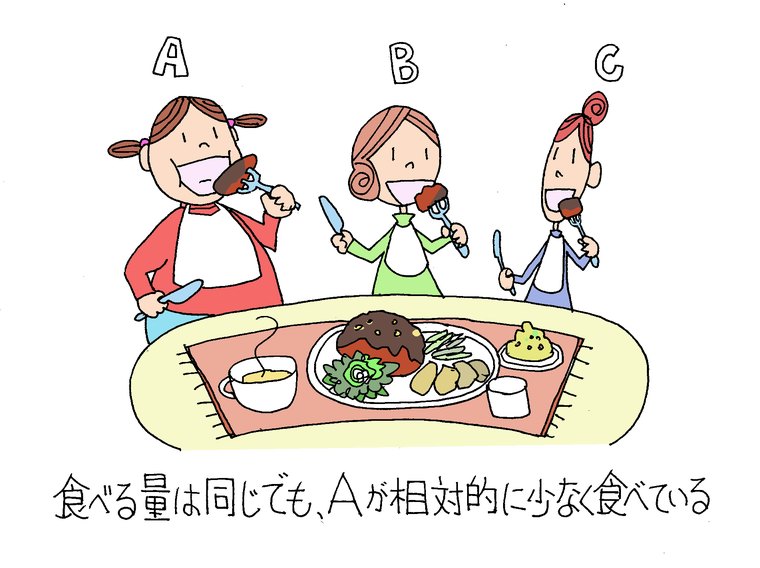
In terms of the food intake, all of them have the same amount and calories, but when we take their weight into account, C, who is forty-five kilograms is eating relatively more, and A, who is ninety kilograms is eating a relatively light meal.
It’s because A who is ninety kilograms has a body twice as large as C, with a thicker chest and a bigger stomach. You can also say that she might have a stronger digestive ability compared to B or C.
Here, when we focus on body size, you can say, “A is eating quantitatively less." When we focus on digestive ability, “A is eating qualitatively simpler than C.
“Qualitatively” means that those with a stronger digestive ability can digest the same amount of food faster, even if they are the same body size. For example, it's been said that Caucasians generally have stronger digestive enzymes for protein and fat, compared to many Asian people.

Now, suppose A orders a large bowl of rice. Regarding intake amount, you might think, “after all, she must be fat because she eats a lot.”
However, if we take their weight into account, since rice is a carbohydrate which is easy to digest, it can be said that A is still eating relatively less and eating a lighter meal compared to B or C.
The bottom line
(1) Based on my intestinal starvation theory, people who have a bigger body or stronger digestion eat relatively less or lighter meals compared to thin people. They are more likely to feel hungrier, and depending on what they eat, they are prone to inducing intestinal starvation and gain more weight.
(2) Also, assuming that European, American, or African people generally have a stronger digestion for fat and protein compared to many Asian people, they are more likely to gain weight than many Asians, even if everyone eats the same. It’s not that they have particular obesity gene.
2017.06.10
Dieting (Eating Less and Exercising More) Doesn’t Work in the Long Run
-
Contents
-
- It has nothing to do with lack of willpower
- What was the long-term effect of dieting
- Cognitive dissonance
It is said that exercising and food restriction is necessary for losing weight. However, we rarely meet those who succeeded in dieting using such a method.
Japanese wrestler Bull Nakano (below) has repeatedly dieted and rebounded, but after having knee problems, it was imperative that she lose weight, so she had a gastrectomy to remove part of her stomach.
She said that “cutting the amount of foods and exercising didn’t make her thinner.”

Japanese comedian, Sugi-chan lost seven kilograms with Billy’s Boots Camp diet method, but rebounded to the same weight afterward.
In this article, I would like to introduce how conventional calorie-based diets are ineffective, based on two books: "Escape the Diet Trap" and "Why Do We Get Fat.”
Please note that most of these are quotations.
1.It has nothing to do with lack of willpower
"Ideas about what causes obesity vary. But you'll almost certainly be familiar with the idea that, at the end of the day, the problem is a product of caloric imbalance: specifically, the consumption of calories in excess of those burned through metabolism and activity. No doubt you'll also be familiar with the idea that the solution to your weight problem is simply to redress the balance by eating less and exercising more.
This advice seems to make sense. The trouble is, not only our collective experience but scientific research, too, shows that applying this advice hardly ever brings significant weight loss in the long term.
The usual explanation offered here is that those who fail with conventional tactics lack willpower and self-control. The reality, though, is that calorie-based strategies for slimming not only don't work, but simply can't work, for all but a small minority.
‘Escape the Diet Trap’ explores the reasons why traditional approaches to weight loss are a crashing failure. It reveals how eating less and exercising more causes the body to resist weight loss, and can actually predispose to weight gain over time."
(Jone Briffa. 2013. Escape the Diet Trap. Pages 1, 19.)
2.What was the long-term effect of dieting
"Limiting the studies to those where individuals were monitored for at least two years after the start of their efforts to lose weight allows us to assess the long-term success of these approaches. Many of us will know what it is to get a short-term win from eating less and exercising more but it's the long game we're interested in here.
<Study1>
Individuals with an average age of 36 and average BMI of 35.0 were prescribed a calorie-reduced diet (individuals ate about 1,000 calories less each day than the amount needed to maintain a stable weight).

Some of the individuals added exercise to this dietary restriction in the form of brisk walking for 45 minutes, 4-5 times each week.
The intervention lasted for a year, and weight was assessed another year after the end of the intervention.

Two years after embarking on a long-term (lasting at least a year) restrictive dietary regime, average weight loss was in the order of just 2 kg. Even when regular exercise is added, the weight loss still only averaged about 3 kg (about 6 lbs).
These outcomes look even more paltry when put in the context of the weight of many of the study participants. For someone of average height, a BMI of 35 works out at about 16 stone. I'd say it's unlikely that individuals of this weight would view a loss of a few pounds as a satisfying return on investment in terms of their diet and exercise efforts.
Another potential surprise is just how ineffective exercise was for the purposes of weight loss when employed as an adjunct to dietary restraint. The results from these studies suggest an additional loss of a mere 1 kg in those who were exercising regularly."
(Briffa. Escape the Diet Trap. Pages 20, 22-3.)
"Prescribing low-calorie diets for obese and overweight patients, according to a 2007 review from Tufts University, leads, at best, to “modest weight losses” that are “transient” – that is, temporary. Typically, nine or ten pounds are lost in the first six months. After a year, much of what was lost has been regained.
The Tufts review was an analysis of all the relevant diet trials in the medical journals since 1980. The single largest such trial ever done yields the very same answer. The researchers were from Harvard and the Pennington Biomedical Research Center, which is in Baton Rouge, Louisiana, and is the most influential academic obesity-research institute in the United States.
Together they enrolled more than eight hundred overweight and obese subjects and then randomly assigned them to eat one of four diets. These diets were marginally different in nutrient composition (proportions of protein, fat, and carbohydrates), but all were substantially the same in that the subjects were supposed to undereat by 750 calories a day, a significant amount.

The subiecte were also given “intensive behavioral counseling” to keep them on their diets, the kind of professional assistance that few of us ever get when we try to lose weight.
They were even given meal plans every two weeks to help them with the difficult chore of cooking tasty meals that were also sufficiently low in calories.
The subjects began the study, on average, fifty pounds overweight. They lost, on average, only nine pounds. And, once again, just as the Tufts review would have predicted, most of the nine pounds came off in the first six months, and most of the participants were gaining weight back after a year.
No wonder obesity is so rarely cured. Eating less –that is, undereating–simply doesn't work for more than a few months, if that."
(Gary Taubes. 2011. Why We Get Fat. Page 36-7.)
3.Cognitive dissonance

"This reality, however, hasn't stopped the authorities from recommending the approach, which makes reading such recommendations an exercise in what psychologists call “cognitive dissonance,” the tension that results from trying to hold two incompatible beliefs simultaneously.
Take, for instance, the Handbook of Obesity, a 1998 textbook edited by three of the most prominent authorities in the field–George Bray, Claude Bouchard, and W. P. T. James.
“Dietary therapy remains the cornerstone of treatment and the reduction of energy intake continues to be the basis of successful weight reduction programs," the book says.
But it then states, a few paragraphs later, that the results of such energy-reduced restricted diets "are known to be poor and not long-lasting.” So why is such an ineffective therapy the cornerstone of treatment? The Handbook of Obesity neglects to say."
(Taubes. Why We Get Fat. Page 37.)