
Topics
02/08/2024
Diabetes (Dysglycemia) is Increasing Despite Decreased Carbohydrate Intake
Contents
- Trends in carbohydrate, fat, and energy intake in Japan(1955-2019)
- Background of the increase in dysglycemia in my opinion
<The bottom line>
If you haven't read the following article yet, please click here to read the original article.
A Low-Carb Diet in Japan:Reducing Carbohydrates Alone is Not the Only Crucial Factor
In this article, I will discuss the causes and background of the relationship between carbohydrate (sugar) intake and the risk of developing diabetes, dysglycemia, etc. in my own way. (The issue of obesity is not discussed in this article.)
1. Trends in carbohydrate, fat, and energy intake in Japan(1955-2019)
First, based on the National Health and Nutrition Survey conducted by the Ministry of Health, Labour and Welfare, the daily intake of carbohydrates, fat, and calories among the Japanese are shown below.
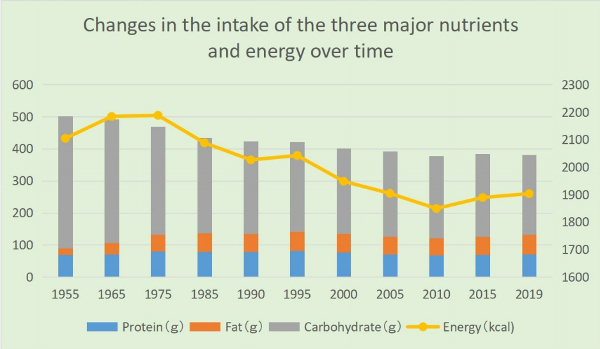
・Carbohydrate intake was 411g in postwar 1955, accounting for 78.1% of total energy intake, but it has been declining since then, reaching 280g in 1995 and 248g (52.1% of total energy intake) in 2019.
・As the economy developed in the postwar period, fat intake sharply increased to 50.1g in 1972 but has remained relatively stable around 55g since 1975. Although there was a slight decrease around the year 2000, annual variations after 1975 are not significant.
・Daily energy intake also increased from 2104 kcal in 1955 to 2287 kcal in 1971. However, there has been a decreasing trend since then, reaching 1903 kcal in 2019.
Nevertheless, the number of diabetes patients and those with blood sugar abnormalities continues to rise. The estimated number of diabetes patients (including those strongly suspected of having diabetes [*1]) has been steadily increasing since the survey began in 1997, from 6.9 million to 10 million in 2016.
If pre-diabetics [*2] with abnormal blood sugar are included, the number surpassed 20 million in 2016 (approximately one in six people). (From the 2016 "National Health and Nutrition Survey" in Japan).
[*1] Individuals with an HbA1c level of 6.5% or higher are considered to be "strongly suspected of having diabetes."
[*2] Individuals with an HbA1c level of 6.0% or higher but less than 6.5% are determined to have a "latent diabetes.”
2. Background of the increase in dysglycemia in my opinion
As evident from the above data, the increase in diabetes patients and individuals with blood sugar abnormalities in Japan cannot be solely explained by carbohydrate or caloric intake.
According to Dr. Yamada, the advocate of the low-carb diet, Japanese people have a weaker ability to secrete insulin than Westerners, and many people can have abnormal blood sugar level even if they are not overweight, but other factors I consider are as follows.
(1) Decline in physical activity
As many experts have pointed out, the increase in diabetes patients and those with blood sugar abnormalities is thought to be partially attributed to a decline in physical activity due to the widespread use of PCs, smartphones, video games, etc. (As for obesity, my theory is that decreased physical activity is not directly related to weight gain or obesity.)
(2) Statistical issues
■The National Health and Nutrition Survey selects about 6,000 households by stratified random sampling from designated unit areas. However, in the 2019 survey, it was reported that cooperative households amounted to 2,836, with 5,900 individuals. Since participation is voluntary, there is a tendency for less cooperation among groups such as men, young people, and singles[1].
■There may be a large gap between the upper and lower limits hidden in the averages. While some people follow an ideally balanced diet, others exhibit poor eating habits. In terms of carbohydrate intake, while some people eat fewer carbs due to dieting, people at high risk of lifestyle-related diseases may be consuming excessive amounts of carbs or have an unbalanced diet that leans toward instant foods, fast foods,etc.
(3) Meal frequency, timing, and more

Not only the quantity and quality of meals but also the frequency, timing, and order of consumption can impact absorption.
Skipping breakfast and having only two meals a day, even with the same amount of carbs at lunch, is said to increase absorption rates, causing a rapid rise in blood sugar levels after lunch.
In contrast, if you consume foods rich in dietary fiber,etc. at breakfast, it can have an impact on the post-lunch and subsequent meal (second meal) blood sugar elevation. This is known as the "second meal effect," as introduced by Dr. Jenkins from the University of Toronto, in 1982.
(4)Dietary balance
■Maintaining a balanced diet is important. Combining carbohydrates with other food groups such as meat, fish, oils, dairy products, and vegetables (fiber) will prolong gastric retention and moderate sugar absorption. This combination may help in controlling the rapid spike in blood sugar levels even with the same amount of carbohydrates. The tendency of many people to reduce fat intake in order to avoid gaining weight may lead to an increase in individuals with abnormal blood glucose levels as well as obesity.
■Since the 1970s, the rise of nationwide fast-food chains and franchise outlets in the food industry has increased opportunities for quick, convenient meals (such as beef bowls, curry, ramen, and hamburgers). These meals often lack vegetables and consist mainly of carbohydrates, potentially leading to a higher risk of blood sugar spikes.

In addition, many Japanese like to eat carbohydrates. Many set menus combine different types of carbohydrates (rice and wheat products), such as ramen noodles and fried rice.
Even if the amount of carbohydrates is small, combinations such as a rice ball and a snack bread (or instant noodles) can easily raise blood glucose levels.
(5) Quality of carbohydrates
■According to statistics from the Ministry of Agriculture in Japan, the per capita annual consumption of rice peaked at 118 kg in 1962 and has since been on a declining trend. By 2020, the consumption had decreased to less than half, reaching 50.8 kg. In addition, examining trends in annual expenditures per household, the amount spent on bread has exceeded the amount spent on rice since 2014.
While the consumption of rice has sharply decreased in recent years, it's crucial to note that there has likely been an increase in the intake of other carbohydrates that raise blood sugar levels, such as bread, sweets, candies, and soft drinks. Thus, relying solely on data related to “carbohydrate intake” may not provide a comprehensive understanding of the situation. (Reference: Japan Low-Carbohydrate Diet Study Group)

■In this context, the glycemic index (GI), which is quantified by blood glucose level and duration after ingesting a food containing 50 g of carbohydrate, is useful.
In addition, there is another indicator called Glycemic Load (GL), which is calculated by multiplying the percentage of carbohydrates in the target food by the GI value.
From the perspective of suppressing a rapid increase in postprandial blood sugar levels, it is important to focus on foods with a low GI/GL value(*3).
While foods such as white bread, refined rice, boiled potatoes, waffles, and french fries,etc are considered to have high GI values, it is worth noting that, foods like unpolished rice, wholegrain bread, beans, and nuts,etc. have low GI values.
(*3) It is said that foods that cause a rapid surge in blood sugar levels, like sugar, but quickly drop, cannot be adequately represented by the GI value.
■It is known that some starches in food, referred to as “resistant starch,” reach the large intestine without being digested. For instance, some starches found in rice, potatoes, and pasta, after being heated and gelatinized, undergo a structural change when cooled, with a portion turning into resistant starch.
Until around the 1970’s to 1980’s when insulated jars were not as common as they are today, it's likely that many people consumed even more resistant starch from "cooled rice" than they do now.
■In the late 1990’s, the National Cancer Center in Japan conducted a five-year follow-up study to investigate the association between carbohydrate intake and the incidence of typeⅡdiabetes. The study targeted approximately 65,000 men and women aged 45 to 75 with no history of diabetes, cardiovascular diseases, or cancer.
According to the findings, in women, there was a higher incidence of diabetes among those with higher intake of simple carbohydrates (sugar, fructose, etc.) and starches[2].
(6)Evolution of cooking, processed foods, etc
■In recent years, advancements in cooking techniques and the proliferation of processed foods have led to a softening of all types of food, including meat, fish, and vegetables, making them melt in the mouth. In my opinion, such foods, being quickly digested with reduced gastric retention time, may potentially accelerate the absorption of carbohydrates.
■Additionally, many processed foods and sweets often utilize artificial sweeteners. While these sweeteners themselves do not raise blood sugar levels, some experts suggest that their habitual use may impact glycometabolism through changes in taste preferences and alterations in gut microbiota [3][4].
The bottom line
(1) In Japan, since the 1955 statistics, carbohydrate intake has consistently decreased. Caloric intake has also been decreasing over the past fifty years. At least in Japan, the recent increase in diabetes patients and those with blood sugar abnormalities is not solely attributed to carbohydrate or caloric intake.
(2) When it comes to carbohydrates, the way blood sugar levels rise varies. The rapid westernization of the Japanese diet since around 1970 has resulted in a drop in rice consumption in Japan to less than half of its peak level in 1962. Instead, it is thought that the intake of processed wheat products (such as bread, noodles, and snacks) and sugar (sweets and soft drinks), which easily raise blood glucose levels, has increased.
Rice is a grain, and therefore the digestive process should be relatively slower compared to flour-based products, etc. However, even the same type of rice can raise blood glucose levels differently depending on the degree of milling, the cooking method, and the cooling method.
(3) I believe that how blood glucose levels rise is also heavily influenced by dietary balance, the frequency and timing of meals, order of intake, and other dietary habits.
For instance, I suspect that a diet that leans towards easily digestible carbohydrates, frequent intake of sugar, and eating habits such as skipping breakfast or fast eating can increase the frequency of insulin secretion, cause sharp fluctuations in blood sugar levels, and place a burden on the pancreas, even if the carbohydrate intake is not that high.
(4) In order to lower the risk of glucose abnormalities, isn't it important to be aware of not only the carbohydrate content of foods, but also how blood sugar levels rise, such as indicated by the Glycemic Index (GI) and Glycemic Load (GL)?
Reducing the intake of high-GI foods and sugars, and opting for low-GI foods (whole grains, protein-rich foods like meat and fish, nuts, dairy), oils, and non-starchy vegetables, is crucial to reduce overall dietary blood sugar elevation.
It's also known that eating regularly three times a day, starting with vegetables, and consuming cooled rice (resistant starch) can contribute to a gentler increase in blood sugar levels throughout the day.
(5) My personal opinion is that a traditional, well-balanced Japanese diet, with rice as the staple, is less likely to increase the risk of obesity and blood sugar abnormalities. Despite the fact that Japan is blessed with seasonal vegetables, seafood, and traditional fermented foods, I feel that in recent years more and more people are eating high GI carbohydrates, meat products, and instant foods, etc.
(For a comprehensive understanding of the effects of low-carb diets, including their impact on obesity causes, please refer to the following article.)
[Related article] A Low-Carb Diet in Japan:Reducing Carbohydrates Alone is Not the Only Crucial Factor
<References>
[1] Japan Society For The Study Of Obesity. Guidelines for the Management of Obesity Disease 2022. Life Science Publishing Co, Dec.2022, Page28.
[2] Kanehara R et al. Association between sugar and starch intakes and type 2 diabetes risk in middle-aged adults in a prospective cohort study. Eur J Clin Nutr. 2022 May;76(5):746-755. doi: 10.1038/s41430-021-01005-1. Epub 2021 Sep 20. PMID: 34545214.
[3] Pepino MY, Bourne C. Non-nutritive sweeteners, energy balance, and glucose homeostasis. Curr Opin Clin Nutr Metab Care. 2011 Jul;14(4):391-5. doi: 10.1097/MCO.0b013e3283468e7e. PMID: 21505330; PMCID: PMC3319034.
[4] Suez, J., Korem, T., Zeevi, D. et al. Artificial sweeteners induce glucose intolerance by altering the gut microbiota. Nature 514, 181–186 (2014). https://doi.org/10.1038/nature13793